“Transfusion-associated graft-versus-host disease (TA-GVHD) is a possible complication of blood transfusion that occurs when viable donor T cells proliferate and engraft in immunodeficient patients after transfusion.”1 It is a delayed, serious and life-threatening reaction occurring later than 24 hours after the start of the transfusion.
“It is far better for this disease to be prevented than to be diagnosed or cured.”
„
Signs and Symptoms
TA-GvHD develops 4−30 days after the transfusion is completed. Clinical symptoms include: fever, maculopapular rash, generalised erythroderma, toxic epidermal necrolysis, vomiting, abdominal pain, diarrhoea, coughing, pancytopenia, electrolyte imbalance or aplastic bone marrow.2
“Mortality in TA-GVHD is estimated to be between 90% and 100%. According to criteria devised by the National Health and Safety Network (NHSN), the diagnosis of TA-GVHD is based on a combination of characteristic clinical findings and a tissue biopsy consistent with GVHD with imputability established via the demonstration of leukocyte chimerism (cells of more than one person in one body, more than one set of DNA), specifically donor “3
What factors influence TA-GvHD?
The severity of the disease is strongly influenced by these three factors:
- the degree of immunological status of the patient
- the degree of HLA similarity
- the number of donor cells in the blood components 4
“Development of TA-GvHD requires that the blood products contain immunocompetent cells. Importantly, the recipient must express tissue antigens absent in the donor and the recipient must also be incapable of mounting an effective immune response to destroy the foreign cells. In cases of TA-GvHD, donor cells replicate and attack the recipient (host), who in turn is unable to mount an adequate immune response.” 5
Who is at risk?
The following main groups of patients are traditionally thought of as at-risk groups and viable cells may trigger the disease in the following recipients:
- Patients on immunosuppressive drugs
- Newborns (poorly developed immune system)
- Recipients with immunodeficiency
- Intrauterine transfusion
- Component for transfusion is from close family member of recipient (HLA-like products)
In these conditions the patients are immunocompromised and may not recognise foreign viable cells in the transfused blood. Immune cells in the transfused blood then attack the tissues of the host – often with fatal outcomes. 6
How to prevent TA-GvHD?
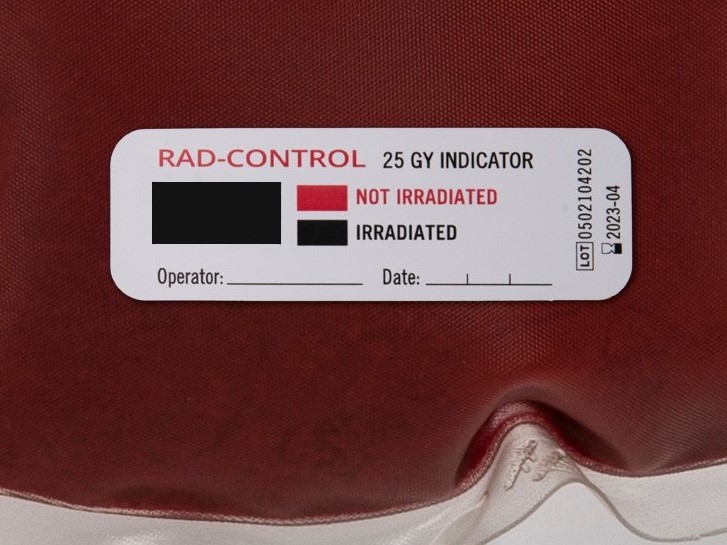
The latest SHOT report with no fatalities due to TA-GvHD in 2020 is the best proof that it is far better for this disease to be prevented than to be diagnosed or cured: TA-GvHD is almost always fatal, with a lower than 10% survival rate. The most common method for preventing TA-GvHD is irradiation of blood components to inactivate residual cells. “Gamma rays and X-rays are similar in their ability to inactivate T cells in blood components at a given absorbed dose.”7
“Various studies have shown that the effect of irradiation on cells is dose dependent: 5 Gy eliminates cell proliferation, 15 Gy results in an 85% to 90% reduction in mitogen response, and 50 Gy results in a 95% to 98.5% reduction in mitogen response. Although a minimum dose of 15 Gy causes DNA breakage and prevents T cell proliferation, the recommended transfusion practice in the United States is that the centre of a component bag should receive 25 Gy (versus 50 Gy in some countries), and any other area outside the bag centre should receive a minimum of 15 Gy (versus 25 Gy in some countries).” 8
For more detailed information, Theodora Foukaneli and a number of co-authors published an update on the use of blood component irradiation to prevent TA-GvHD in 2020, on behalf of the BSH Transfusion Task Force. 7 We also recommend listening to episode 013 of the Blood Bank Guy Essentials Podcast for more information on TA-GvHD and other transfusion-related complications.
Sources:
Photo: https://rdcu.be/cogx4
1 Sezer Saglam (2011). Blood Irradiation, Modern Approaches To Quality Control, Dr. Ahmed Badr Eldin (Ed.), ISBN: 978-953-307-971-4, InTech, Available from: http://www.intechopen.com/books/modern-approaches-toquality-control/blood-irradiation
2 Dr Juan Klopper: Transfusion Associated Graft Versus Host Disease, Youtube, https://www.youtube.com/watch?v=Pqichuba5CA
3 A systematic review of transfusion-associated graft-versus-host disease: (Blood. 2015;126(3):406-414)
4 Dr. Preeyanat Vongchan, Transfusion associated graft vs host disease (TA-GvHD), Youtube, https://www.youtube.com/watch?v=1e6Jn9_X0kA
5 Aaron E. Pritchard, MD; Beth H. Shaz, MD: Survey of Irradiation Practice for the Prevention of Transfusion-Associated Graft-versus-Host Disease; Arch Pathol Lab Med Vol 140 (10): 1092–1097. |01 October 2016
6 ISBT Science Series (2020) 15, 207-231 © The Author. Journal Compilation © 2020 Blackwell Publishing Ltd. DOI:10.1111/voxs.12598
7 © 2020 The Author. British Society for Haematology and John Wiley & Sons Ltd. British Journal of Haematology, 2020, 191, 704–724, Guidelines on the use of irradiated blood components
8 Burak Bahar, MD; Christopher A. Tormey, MD: Prevention of Transfusion-Associated Graft-Versus-Host Disease With Blood Product Irradiation; Arch Pathol Lab Med—Vol 142, May 2018
Interesting posts

We’re back from an inspiring week at ISBT Milan 2025, where we had the opportunity to connect with leading voices in transfusion medicine from around the world.

Autologous serum eye drops are obtained from the patient's own blood and represent an individualized and highly effective form of treatment for patients with severe eye conditions.

Serum Eye Drops (SED) are highly effective in the treatment of patients suffering from dry eye disease, among other things. You can find out where and how to obtain serum eye drops in Austria here.

On point medicals has won the 2024 Innovations- and Research Award of the Federal State of Carinthia.

Dry eye disease (DED) is a prevalent and often underestimated ocular condition that affects millions of people worldwide. Find out more about causes, symptoms and treatment options.

Serum Eye Drops (SED) are similar to normal tears and show a high efficacy in therapy with patients suffering from severe ocular surface problems, such as Dry Eye Disease. Learn more about this widely unknown blood-derived therapy.

Blood irradiation is vital for patients at risk of developing TA-GvHD. Find out more about how to correctly verify blood irradiation and why dosimetry checks and the use of irradiation indicators should not be ignored or confused.
Blood irradiation is vital for patients at risk of developing TA-GvHD. Find out more about how to correctly verify blood irradiation and why dosimetry checks and the use of irradiation indicators should not be ignored or confused.

Cold chain management can ensure that unused blood products are returned to the blood bank safely. In times of blood shortages it is more than important that surplus blood products can be reused. More on why temperature monitoring is essential.
![[:de]Blutbesstrahlung vor einer Transfusion verhindert TA-GvHD[:en]Blood irradiation prior to transfusion prevents TA-GvHD[:]](https://onpointmedicals.at/wp-content/uploads/2021/11/What-is-blood-irradiation-scaled.jpg)
Blood is irradiated before transfusion in order to avoid the formation of the rare but mostly fatal TA-GvHD. Here is why it is much better to prevent this disease with blood irradiation than to diagnose it.
